BACKGROUND: Although bariatric surgery is the fastest and most effective way to lose and control weight, some overweight patients are not eligible for this procedure. Endoscopic placement of a Silicone Intragastric Balloon (SIB) to restrict gastric intake in obese patients is a cheaper and less invasive alternative to bariatric surgery, bringing about significant weight loss. Placement and removal of SIBs has so far been carried out in a hospital setting, often under general anesthesia, which increases procedure costs.
AIM: To report improvements made in the technique for office placement and removal of SIBs.
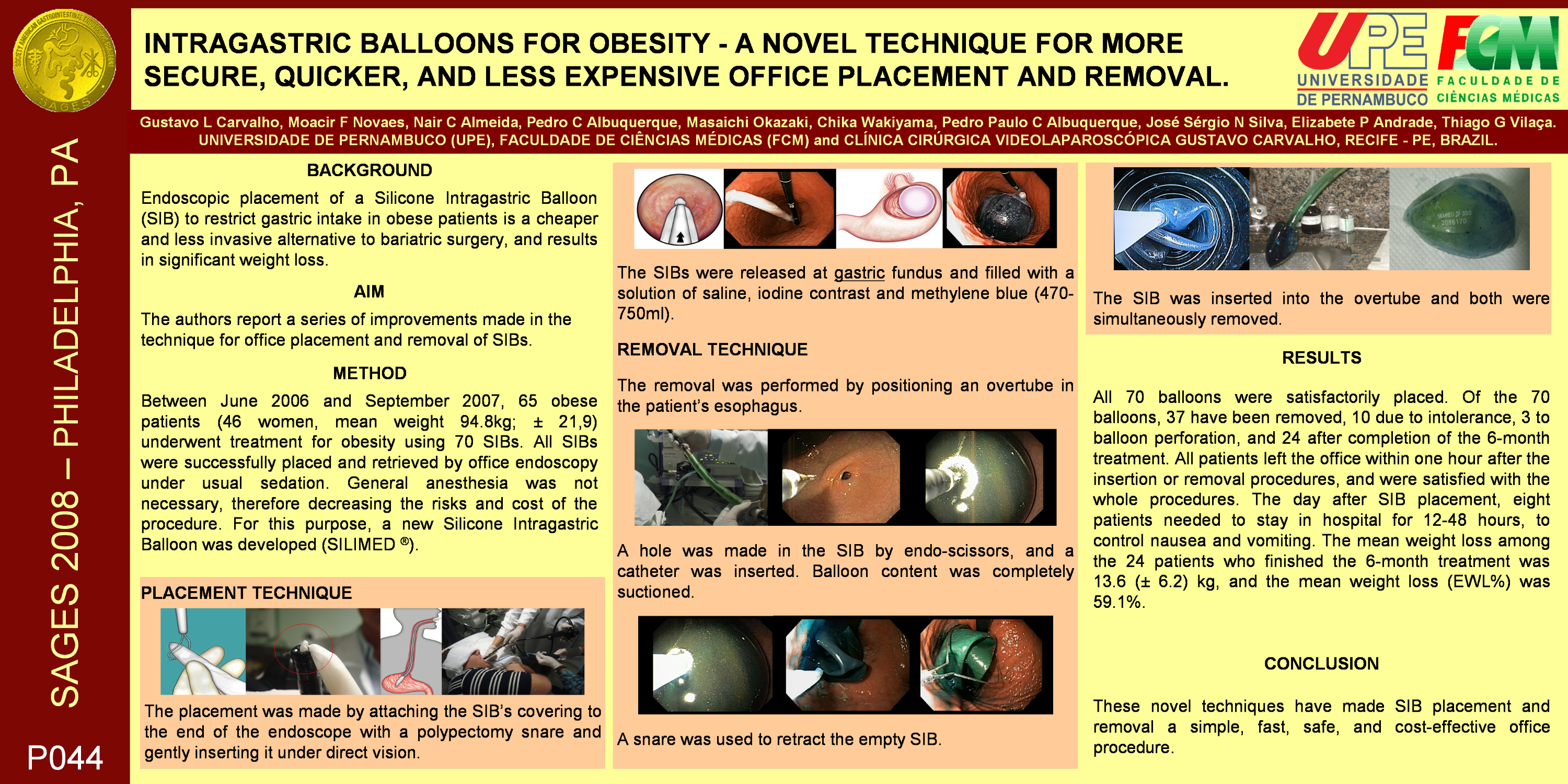
METHOD: Between June 2006 and September 2007, 65 obese patients (46 women, Average weight 94.8kg; ± 21,9) underwent treatment for obesity using 70 SIBs. All SIBs were successfully placed and retrieved by way of office endoscopy under normal sedation. General anesthesia was not necessary, thereby greatly decreasing the risks and the cost of the procedure. For this purpose, a new Silicone Intragastric Balloon was developed (SILIMED ®). Placement was carried out by attaching the specially designed SIB covering to the end of the endoscope with a polypectomy snare and gently inserting it under direct vision. The SIBs were released at the stomach fundus and filled with a solution of saline, iodine contrast and methylene blue (470-800ml). Retrieval was performed by positioning an overtube in the patient’s esophagus. A hole was made in the SIB using a needle or endo-scissors, and a catheter was inserted. The entire contents of the balloon were removed using suction, completely emptying the SIB. A snare was used to retract the empty SIB. The SIB was inserted into the overtube and both were removed together.
RESULTS: All 70 balloons were satisfactorily placed. Of the 70 balloons, 37 have since been removed, 10 because of intolerance, 3 through balloon perforation, and 24 at the end of the 6-month course of treatment. All patients left the office within one hour after the insertion or removal procedures, and were satisfied with the procedure and the sedation. The day after SIB placement, eight patients needed to stay in hospital for 12-48 hours, to control nausea and vomiting. The average weight loss among the 24 patients who finished the 6-month course of treatment was 13.6 (± 6.2) kg, and the average excessive weight loss (EWL%) was 59.1%.
CONCLUSION: These novel techniques have made SIB placement and removal an office procedure, which is fast, safe, and cost-effective.
Session: Poster
Program Number: P044

{kind=link}