Jennifer J Freeman, MD, Alexander Feliz, MD, Shawn Tsuda, MD. University of Nevada School of Medicine
Background: Limited retraction has been an obstacle in the advancement of pure transumbilical cholecystectomy. Adequate retraction is essential in obtaining a critical view for safe cholecystectomy. As a result, several groups have investigated alternative methods for fundal retraction, including the use of additional needlescopic (2 mm) or 5 mm ports to assist in obtaining the critical view of safety. We reviewed the results of a single institution with respect to transumbilical cholecystectomy with a single subxyphoid 2 mm needlescopic instrument for retraction of the gallbladder fundus to aid in obtaining a critical view of safety.
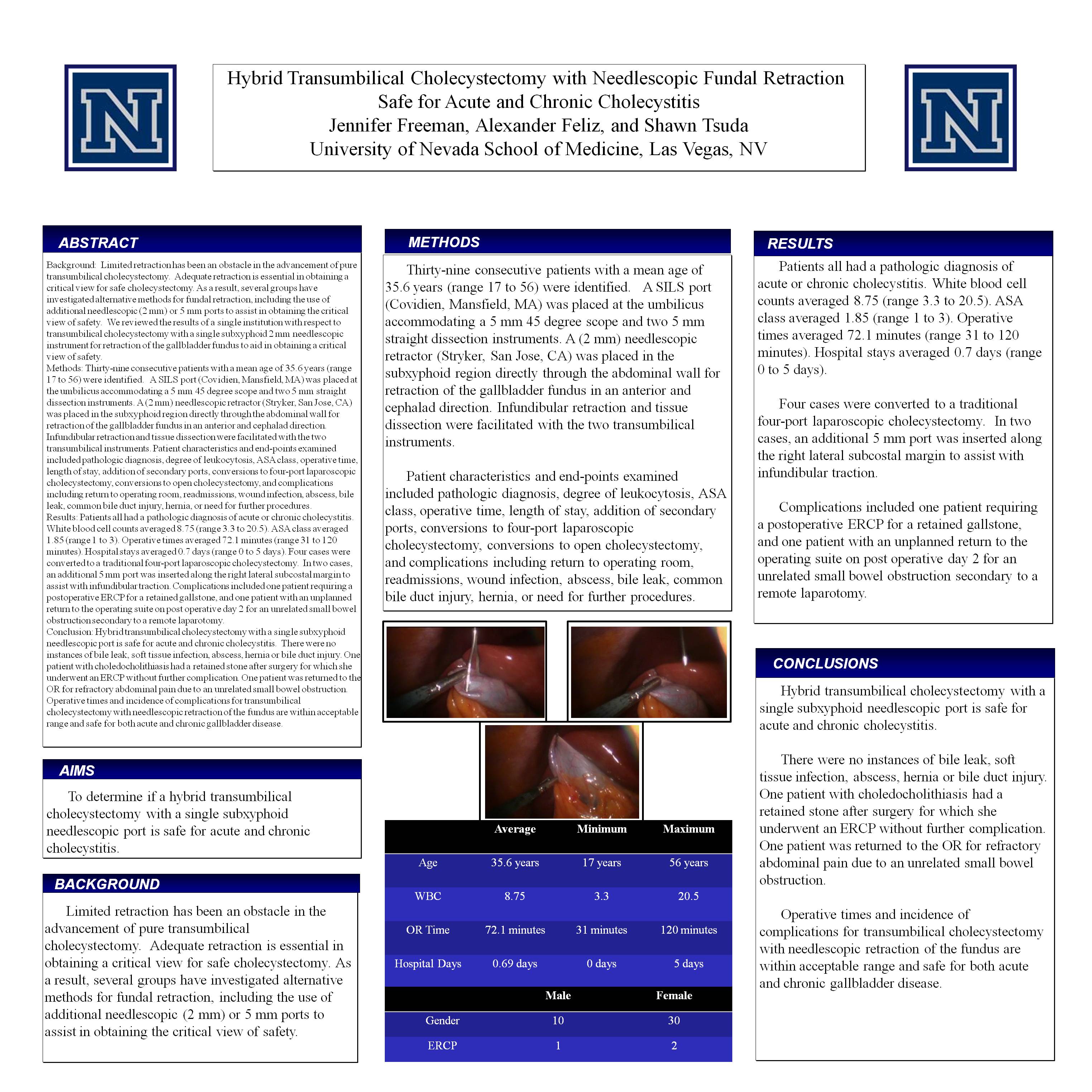
Methods: Thirty-nine consecutive patients with a mean age of 35.6 years (range 17 to 56) were identified. A SILS port (Covidien, Mansfield, MA) was placed at the umbilicus accommodating a 5 mm 45 degree scope and two 5 mm straight dissection instruments. A (2 mm) needlescopic retractor (Stryker, San Jose, CA) was placed in the subxyphoid region directly through the abdominal wall for retraction of the gallbladder fundus in an anterior and cephalad direction. Infundibular retraction and tissue dissection were facilitated with the two transumbilical instruments. Patient characteristics and end-points examined included pathologic diagnosis, degree of leukocytosis, ASA class, operative time, length of stay, addition of secondary ports, conversions to four-port laparoscopic cholecystectomy, conversions to open cholecystectomy, and complications including return to operating room, readmissions, wound infection, abscess, bile leak, common bile duct injury, hernia, or need for further procedures.
Results: Patients all had a pathologic diagnosis of acute or chronic cholecystitis. White blood cell counts averaged 8.75 (range 3.3 to 20.5). ASA class averaged 1.85 (range 1 to 3). Operative times averaged 72.1 minutes (range 31 to 120 minutes). Hospital stays averaged 0.7 days (range 0 to 5 days). Four cases were converted to a traditional four-port laparoscopic cholecystectomy. In two cases, an additional 5 mm port was inserted along the right lateral subcostal margin to assist with infundibular traction. Complications included one patient requiring a postoperative ERCP for a retained gallstone, and one patient with an unplanned return to the operating suite on post operative day 2 for an unrelated small bowel obstruction secondary to a remote laparotomy.
Conclusion: Hybrid transumbilical cholecystectomy with a single subxyphoid needlescopic port is safe for acute and chronic cholecystitis. There were no instances of bile leak, soft tissue infection, abscess, hernia or bile duct injury. One patient with choledocholithiasis had a retained stone after surgery for which she underwent an ERCP without further complication. One patient was returned to the OR for refractory abdominal pain due to an unrelated small bowel obstruction. Operative times and incidence of complications for transumbilical cholecystectomy with needlescopic retraction of the fundus are within acceptable range and safe for both acute and chronic gallbladder disease.
Session: Poster
Program Number: P376
View Poster
{kind=link}