INTRODUCTION: The risk of anastomotic leak in the laparoscopic colorectal resection with the Double Stapling Technique (DST) increases when the endo-linearstapler (ELS) is used more than three times in dividing the distal rectum. The anastomotic breakdown may be caused by the low blood perfusion at the site of gStaple on Stapleh. Therefore, it is important to avoid multi-stapling in dividing the rectum. However, we sometimes experience difficulties in dividing the distal rectum within two ELS in the laparoscopic procedures. These are supposed to correlate with the location or the size of tumor, the width of the pelvic space, the patientfs BMI, and so on. Therefore, we evaluate the way to cope with the difficulties in dividing the distal rectum perpendicularly to the long axis with less than two staplers.
METHODS: The laparoscopic colorectal resection was performed in 138 patients from March 2004 to August 2007. Out of them, 56 patients who underwent a DST anastomosis were retrospectively reviewed, concerning the way of dividing the distal rectum and the outcome.
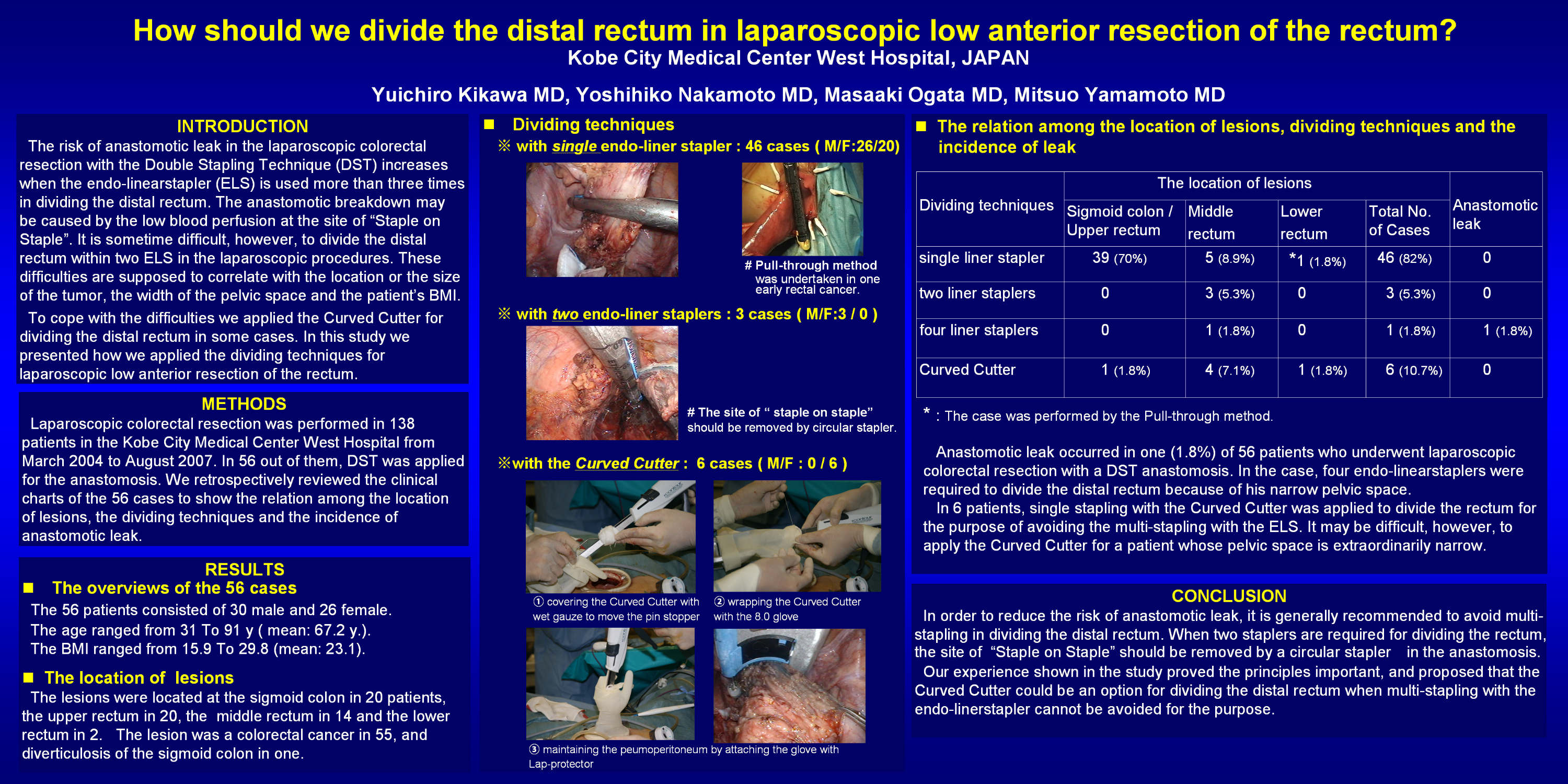
RESULTS: Among the 56 patients (30 male, 26 female), 55 patients had a colorectal cancer and one patient had sigmoid diverticulosis. The locations of the lesions were the sigmoid colon in 20, the upper rectum in 20, the middle rectum in 14 and the lower rectum in 2. In 45 (80%) of 56 patients, the rectum was divided by single ELS. The lesions were all located proximal to the lower rectum, and no anastomotic leak occurred. In 3 male patients (5.3%), two ELS were required for dividing the middle rectum. In the following DST anastomosis, we advanced the center rod of the circular stapler through the site of gStaple on Stapleh. No anastomotic leak occurred in the cases. In one male patient with a narrow pelvic space, however, four ELS were required for dividing the lower rectum and then, anastomotic leak occurred. On the other hand, single stapling with the curved cutter used in the open surgery was adopted in 6 female patients (10.7%), although it was necessary to extend the skin incision to 6cm. No anastomotic leak occurred in the cases. In one female patient with an early rectal cancer of the lower rectum, the pull-through method was undertaken for dividing the rectum by single stapling. No anastomotic leak occurred.
CONCLUSIONS: It is important to avoid multi-stapling in dividing the distal rectum to reduce the anastomotic leak when the DST anastomosis is undertaken. When two ELS are required for dividing the rectum, the site of gStaple on Stapleh should be removed by a circular stapler. When multi-stapling with the ELS cannot be avoided for dividing the distal rectum, the curved cutter can be applied to divide the rectum by single stapling.
Session: Poster
Program Number: P092

{kind=link}