Iswanto Sucandy, MD, Jeffrey Berman, MD, Gintaras Antanavicius, MD FACS. Abington Memorial Hospital
Introduction : In many bariatric centers, nasogastric tube (NGT) is routinely utilized during creation of the gastrojejunal anastomosis in a roux-en-y gastric bypass or the duodenojejunal anastomosis in a duodenal switch. A potential complication of this technique includes inadvertent stapling or suturing of the NGT depending on the type of anastomosis performed (stapled versus handsewn). In this study we describe a successful endoscopic removal of an inadvertently sutured NGT at the level of the duodenojejunal anastomosis during a robotically-assisted laparoscopic biliopancreatic diversion with duodenal switch (R-LBPD/DS).
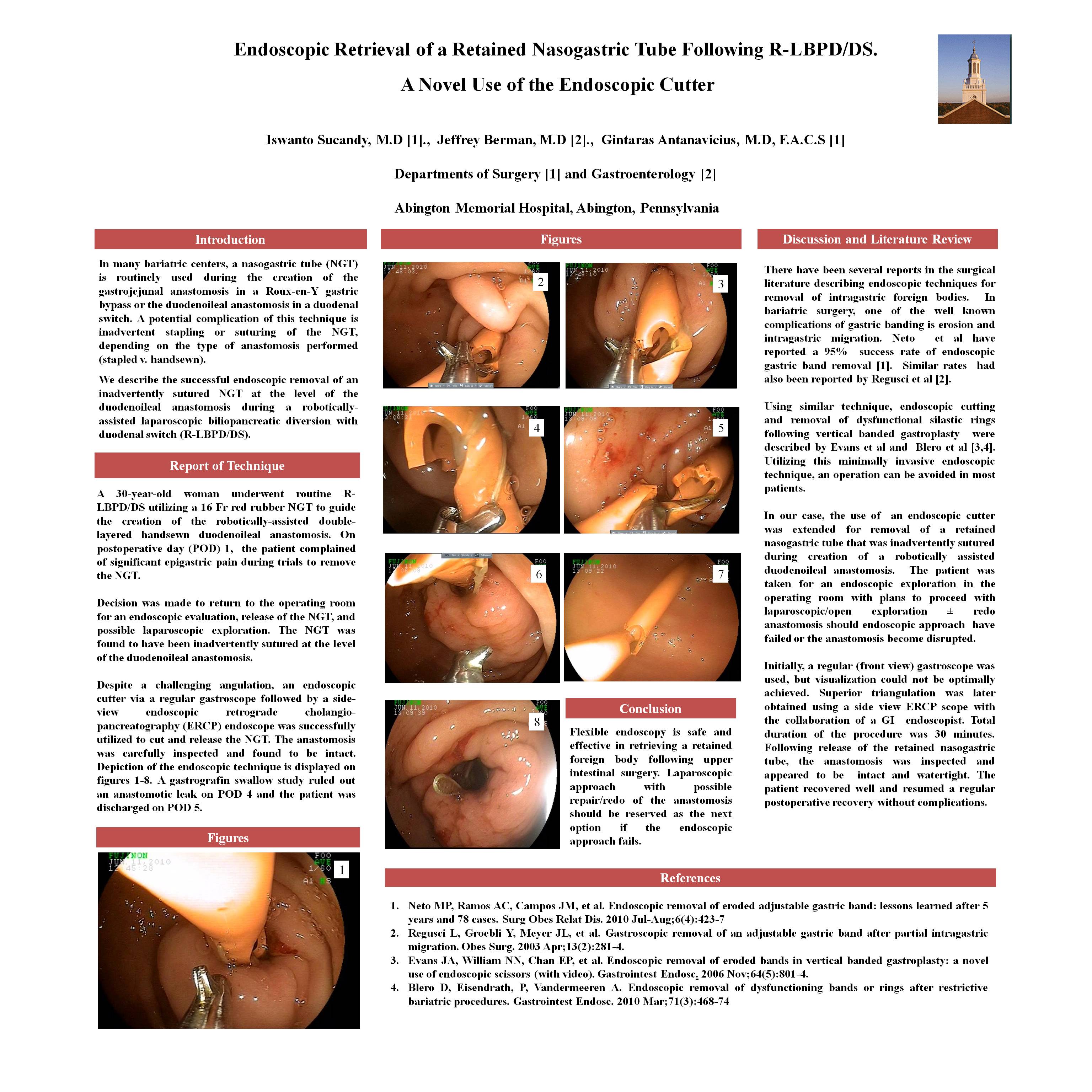
Report of Technique : A 30 year old woman underwent a routine R-LBPD/DS utilizing a 16 Fr red rubber NGT to guide the creation of the robotically-assisted double-layered handsewn duodenojejunal anastomosis. The operation was uneventful however on postoperative day (POD) 1, the patient complained of significant epigastric pain during trials to remove the NGT. Decision was made to return to the operating room for an endoscopic evaluation, release of the NGT, and possible laparoscopic exploration. The NGT was found to be inadvertently sutured at the level of the duodenojejunal anastomosis. Despite a challenging angulation, an endoscopic cutter via a regular gastroscope followed by a side-view ERCP scope were successfully utilized to cut and release the NGT. The anastomosis was carefully inspected and found to be intact. A gastrografin swallow study ruled out an anastomotic leak on POD 4 and the patient was discharged on POD 5.
Conclusions : Flexible endoscopy is safe and effective in retrieving a retained foreign body following an upper intestinal surgery. Laparoscopic approach with possible repair/redo of the anastomosis should be reserved as the next option when the endoscopic approach fails.
Session: Poster
Program Number: P024
View Poster
{kind=link}