Shannon Stogryn, BSc, MBBS, Jennifer Metcalfe, MD, Ashley Vergis, MD, MMEd, FRCSC, FACS, Krista Hardy, MSc, MD, FRCSC. University of Manitoba.
Introduction – Acute cholecystitis (AC) is one of the most common reasons for emergency admission to general surgical services. Ultrasound (US) is the mainstay of biliary tract imaging, but there have been few recent studies that test its ability to diagnose AC. The objective of this study was to determine how well an US diagnosis of AC correlates with intraoperative diagnosis. It is hypothesized that US under calls the frequency and severity of AC in the emergency setting leading to unexpected findings in the operating room.
Methods & Procedures – This retrospective review included all patients admitted to the acute care surgical service of a tertiary hospital in 2011 with suspected biliary pathology who underwent a diagnostic US and subsequent cholecystectomy. Major US indicators used to diagnose AC included cholelithiasis, wall thickening (>3mm), and a positive sonographic Murphy’s sign. Minor indicators included pericholecystic fluid and distension. The sensitivity (sen), specificity (spec), positive predictive value (PPV), and negative predictive value (NPV) of US were determined using the intraoperative diagnosis as the gold standard. Further analysis identified which US indicators were most predictive of an intraoperative diagnosis of AC. A logistic regression model was used to analyze the effect of age, gender, BMI, and diabetes on US reliability.
Results – Of the 288 patients receiving an US for biliary symptoms, 152 were definitively diagnosed with AC and 143 (94%) of these patients underwent emergency surgery (median time to OR = 23.03 hours). The ability of US to predict intraoperative findings is summarized in Table 1. The individual US indicators most predictive of AC are summarized in Table 2.
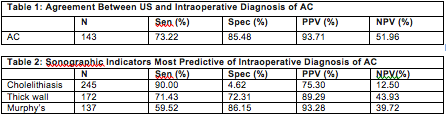
For the 102 patients with other biliary pathology who underwent cholecystectomy, there were 49 with intraoperative findings suggestive of AC (false negative rate of 48.04%). The logistic regression model showed that selected patient demographics had no significant effect on the accuracy of ultrasound diagnosis (BMI: p = 0.2403, age: p = 0.4149, gender: p = 0.6702, diabetes: p = .9407).
Conclusions – US is highly sensitive and specific for diagnosing AC. The poor NPV, however, confirms our hypothesis that US can under call AC. If an US impression of AC is not given, the presence of cholelithiasis, wall thickening and a sonographic Murphy’s sign are most predictive of AC. BMI, age, gender, and diabetes had no effect on the ability of US to correctly diagnose AC.
View Poster