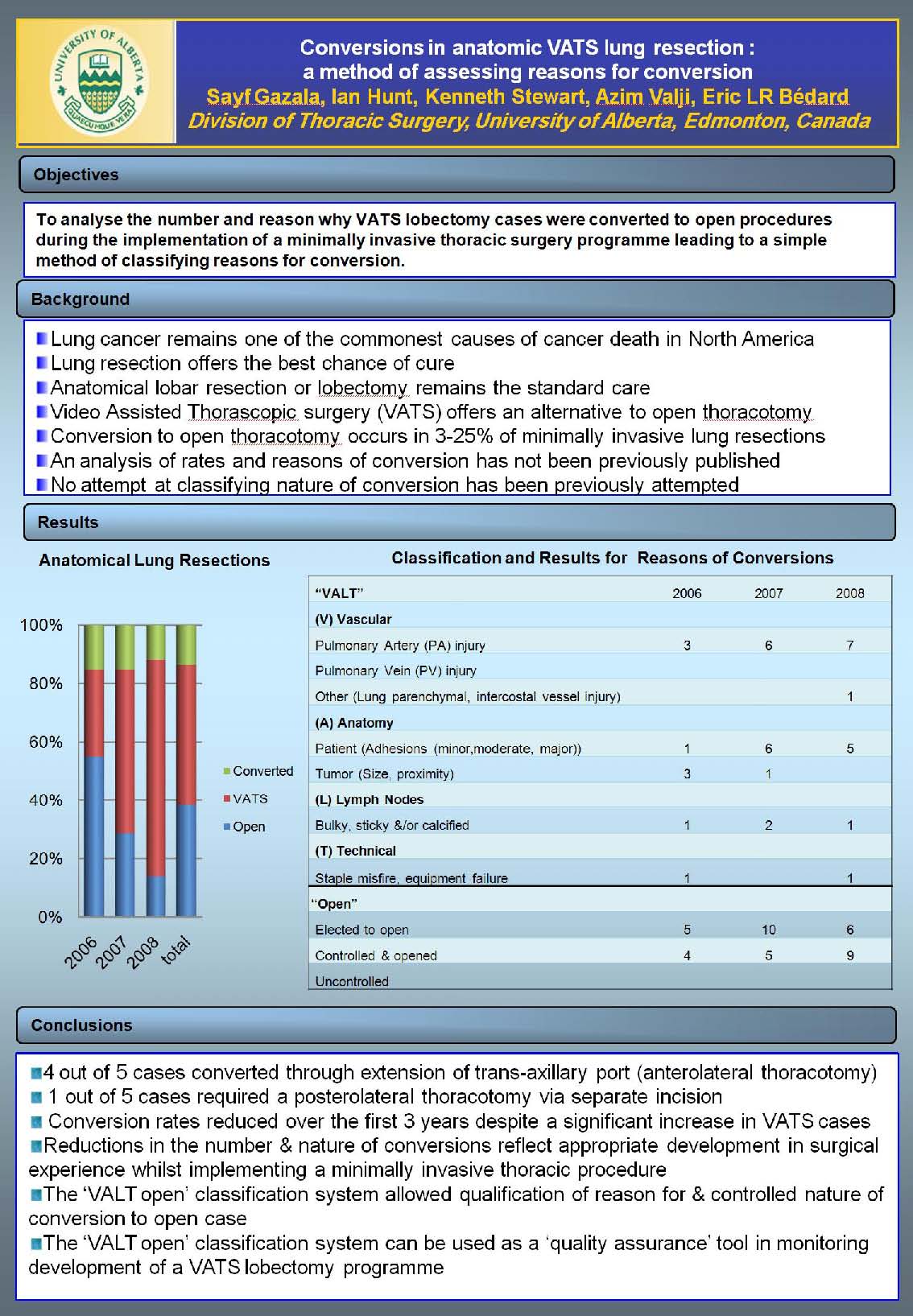
Objectives: Following analysis of why VATS lobectomy cases were converted to open procedures we propose a simple method of classifying reason for conversion that allows monitoring during the implementation & development of a minimally invasive thoracic surgery program. Background: Lung cancer remains one of the commonest causes of cancer death in North America. Lung resection offers the best chance of cure. Anatomical lobar resection or lobectomy remains the standard of care. non-rib spreading,Video Assisted Thorascopic surgery (VATS) offers an alternative to open thoracotomy. Published data would suggest conversion to open thoracotomy occurs in 3-20% of minimally invasive lung resections. An analysis of rates and reasons of conversion has not been previously published Results: 220 consecutive VATS lobectomy cases were analysed. Overall conversion rate was 12.7% over 3years. Conversions were classified according to whether conversion was due to Vascular (V), Anatomic (A), Lymph node related (L) or Technical problems (T) & whether ‘opening (VALTopen)’ was Elective, Controlled or Uncontrolled. 4 out of 5 cases converted through extension of trans-axillary port (anterolateral thoracotomy). 1 out of 5 cases required a posterolateral thoracotomy via separate incision. Conversion rates decreased by 50% over the first 3 years despite a significant increase in VATS cases. The indication for conversion changed with fewer vascular injuries to the Pulmonary Artery & fewer conversions for ‘poor visualization’
Conclusions: Reductions in the number & nature of conversions reflect appropriate development in surgical experience and patient selection while implementing a minimally invasive thoracic procedure. The ‘VALT open’ classification system allowed qualification of reason for & controlled nature of conversion to open case. The ‘VALT open’ classification system can be used as a ‘quality assurance’ tool in monitoring development of a VATS lobectomy program.
Session: Poster
Program Number: P204

{kind=link}