G F Paulus, MD, M van Avesaat, MD, J M Conchillo, MD, PhD, A A Masclee, MD, PhD, N D Bouvy, MD, PhD. Maastricht University Medical Center.
Introduction
Bariatric surgery is the only long-term effective therapy for weight loss in morbidly obese patients and therefore has an increasing role in surgical practice. With the rising number of procedures, research and development of minimal invasive procedures also increases. Recently, our center started a endoscopic method to reduce the volume of the stomach by creating plications. Excess BMI loss of 30.1% after 3 months was presented in last years abstract. A substudy was performed to assess possible mechanisms that lead to this weight loss.
Methods and procedures
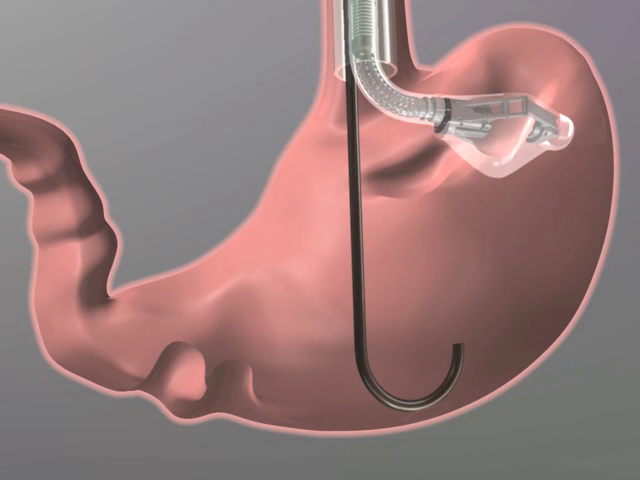
The procedure starts with placing an endogastric tube to secure a safe entry route to the stomach. Through this tube an Articulating Circular Endoscopic (ACE) stapler device is introduced. With the device, stomach tissue is acquired by vacuum and stapled to create eight to ten permanent plications (figure 1). Before and one month after the procedure patients underwent a standardized meal test with blood sampling for gastrointestinal hormones, breath sampling for gastric emptying (13C-octoanoic acid breath test) and visual analogue scale (VAS) for hunger and satiety. Samples were obtained at several time points before and after a standardized breakfast. Changes in weight, hormonal changes and gastric emptying were tested with the paired t-test, VAS scores with repeated measures ANOVA. To analyze hormonal response to the breakfast, incremental areas under the curve (iAUC) for ghrelin, GLP-1 and PYY were computed. For each subject we separately calculated regression slopes, R and R2 values for the correlation between VAS scores and hormone concentrations.
Results
Ten patients underwent the gastric plication procedure and were tested. Baseline weight was 119.3±3.5 kg, which had decreased to 111.6±3.4 kg (p<0.001) at day of the standardized meal test, one month after the procedure. No changes were found in gastric emptying (GE) compared to baseline (GE half time 141.3±5.9 preoperative vs 138.7±12.3 minutes postoperative, p>0.05)
Statistical analysis of Ghrelin concentration in the first hour showed significantly different iAUC after the procedure (6.7±9.1 vs. -33.3±12.0, p<0.05). Furthermore, iAUC of VAS for desire to eat significantly decreased after the procedure (-21.2±7.1 vs. -41.7±7.4, p<0.05).
After the procedure we found a significant correlation (see table 1) between ghrelin levels and desire to eat in the first hour of the test day that did not reach statistical significance before the procedure.
We did not find any significant changes in the anorexigenic hormones GLP-1 and PYY.
One year after plicating the stomach mean weight was 100.3±3.5 kg which is a mean weight loss of 19.0±2.4 kg.
Conclusion
Post-procedural plasma levels of the hunger hormone ghrelin, showed a significant decrease as a response to the meal. This can be related to increased stretch on the plicated fundus. This effect might explain part of the reduced caloric intake as desire to eat changes significantly after the procedure and is positively correlated to plasma levels of Ghrelin.
We emphasize that the changed Ghrelin response is part of the explanation to why patients are more likely to reduce caloric intake and lose a significant amount of weight after plicating the stomach.


View Poster