Venkata K Kella, MD, Navalkishor Udgiri, Carrie Sims, MD FACS. University of Pennsylvania, 3400 Spruce street, Philadelphia. PA 19104
INTRODUCTION: Hydatid disease, caused by the tape worm Echinococcus, results in liver and pulmonary cystic lesions. Although frequently asymptomatic, chronic inflammation from hydatidois can result in portal hypertension and ascites. Chylous ascites, however, is extremely rare and we present the first reported case of abdominal compartment syndrome due to chylous ascites in the setting of hepatic hydatidosis.
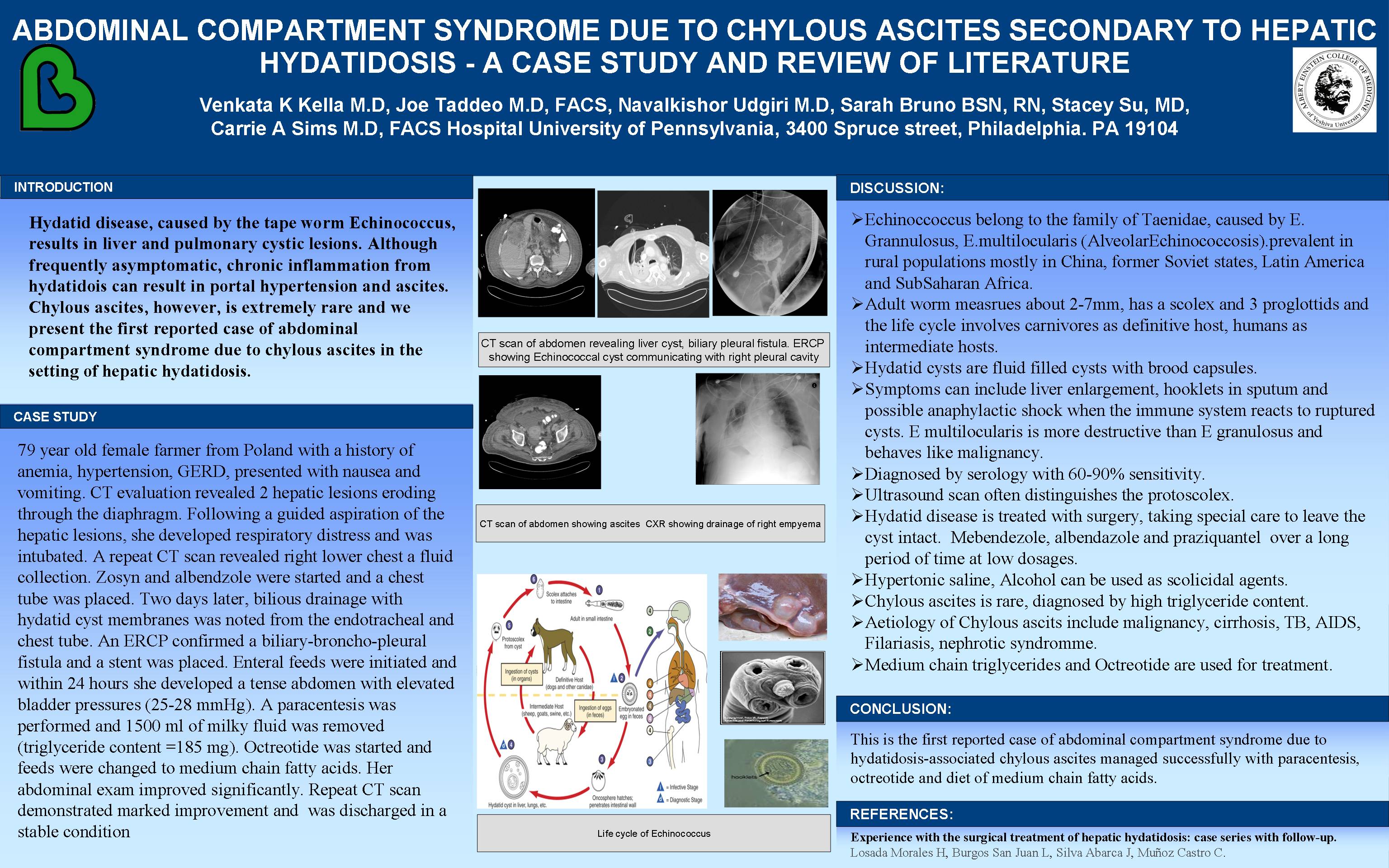
CASE STUDY: 79 year old female farmer from Poland with a history of anemia, hypertension, GERD, presented with nausea and vomiting. CT evaluation revealed 2 hepatic lesions eroding through the diaphragm. Following a guided aspiration of the hepatic lesions, she developed respiratory distress and was intubated. A repeat CT scan revealed right lower chest a fluid collection. Zosyn and albendzole were started and a chest tube was placed. Two days later, bilious drainage with hydatid cyst membranes was
noted from the endotracheal and chest tube. An ERCP confirmed a biliary-broncho-pleural fistula and a stent was placed. Enteral feeds were initiated and within 24 hours she developed a tense abdomen with elevated bladder pressures (25-28 mmHg). A paracentesis was performed and 1500 ml of milky fluid was removed (triglyceride content =185 mg). Octreotide was started and feeds were changed to medium
chain fatty acids. Her abdominal exam improved significantly. Repeat CT scan demonstrated marked improvement. She was discharged in a stable condition.
CONCLUSION: We present the first reported case of abdominal compartment syndrome due to hydatidosis-associated chylous ascites managed successfully with paracentesis, octreotide and diet of medium chain fatty acids.
Session: Poster
Program Number: P373
View Poster
{kind=link}