Amalia Stefanou, MD, John Park, MD, Slawomir Marecik, MD, Leela Prasad, MD. Advocate Lutheran General Hospital, University of Illinois Chicago Hospital, Cook County Hospital
Objective
We present a novel use of flexible stent for the treatment of small bowel stricture in a patient with inflammatory bowel disease. While the use of stents has been accepted in esophageal and in colonic obstructions, they rarely are used in the treatment of small bowel strictures. Stents have mainly been used for malignant or palliative obstruction, with increasing use in benign disease. Literature supporting the use of stents in small bowel pathologies has largely been absent. We present a case of ileoanal pouch anastomotic stricture in a patient with Crohns disease presenting as obstruction and the use of stent placement to avoid further need for operation.
Methods
Patient is a fifty-five year old male who had a presumed history of ulcerative colitis and underwent proctocolectomy with ileoanal pouch anastomosis (IPAA) in 1993. Following this, he developed small bowel obstruction in 2004 and operative small bowel resection was performed for stricturing disease. Pathology from the specimen diagnosed Crohns disease.
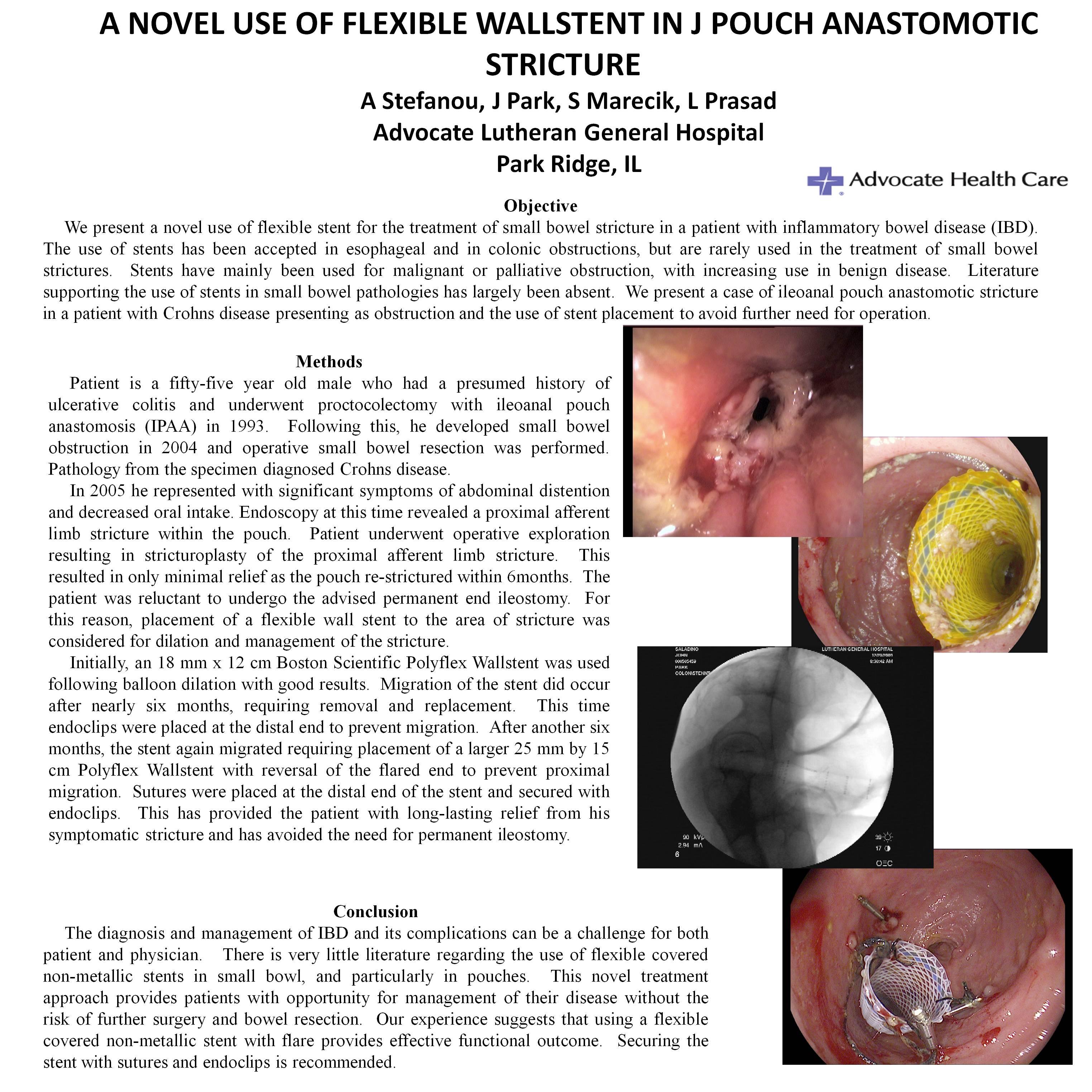
In 2005 he represented with significant symptoms of abdominal distention and decreased oral intake. Abdominal CT scan demonstrated small bowel obstruction. Flexible sigmoidoscopy at this time revealed a proximal afferent limb stricture within the pouch. Patient underwent operative exploration resulting in stricturoplasty of the proximal afferent limb stricture. The stricturoplasty resulted in only minimal relief of symptoms as the pouch re-strictured within 6months. The patient was very reluctant to undergo the advised permanent end ileostomy. For this reason, placement of a flexible wall stent to the area of stricture was considered for dilation and management of the stricture.
Initially, an 18 mm x 12 cm Boston Scientific Polyflex Wallstent was used following balloon dilation with good results. Migration of the stent did occur after nearly six months, requiring removal and replacement. This time endoclips were placed at the distal end to prevent migration. After another six months, the stent again migrated requiring placement of a larger 25 mm by 15 cm Polyflex Wallstent with reversal of the flared end to prevent proximal migration. Sutures were placed at the distal end of the stent and secured with endoclips. This has provided the patient with long-lasting relief from his symptomatic stricture and has avoided the need for permanent ileostomy.
Conclusion
The diagnosis and management of inflammatory bowel disease and its complications can be a challenge for both patient and physician. On review of the literature, there is very little discussion regarding the use of flexible covered non-metallic stents in small bowl, and particularly in pouches. This novel treatment approach provides patients with opportunity for management of their disease without the risk of further surgery and bowel resection. Our experience suggests that using a flexible covered non-metallic stent with flare provides effective functional outcome. Securing the stent with sutures and endoclips is recommended.
Session Number: Poster – Poster Presentations
Program Number: P630
View Poster