Filippo Filicori, MD, Xavier M Keutgen, MD, Thomas J Fahey III, MD FACS, Rasa Zarnegar, MD FACS. Department of Surgery, Weill Cornell Medical College
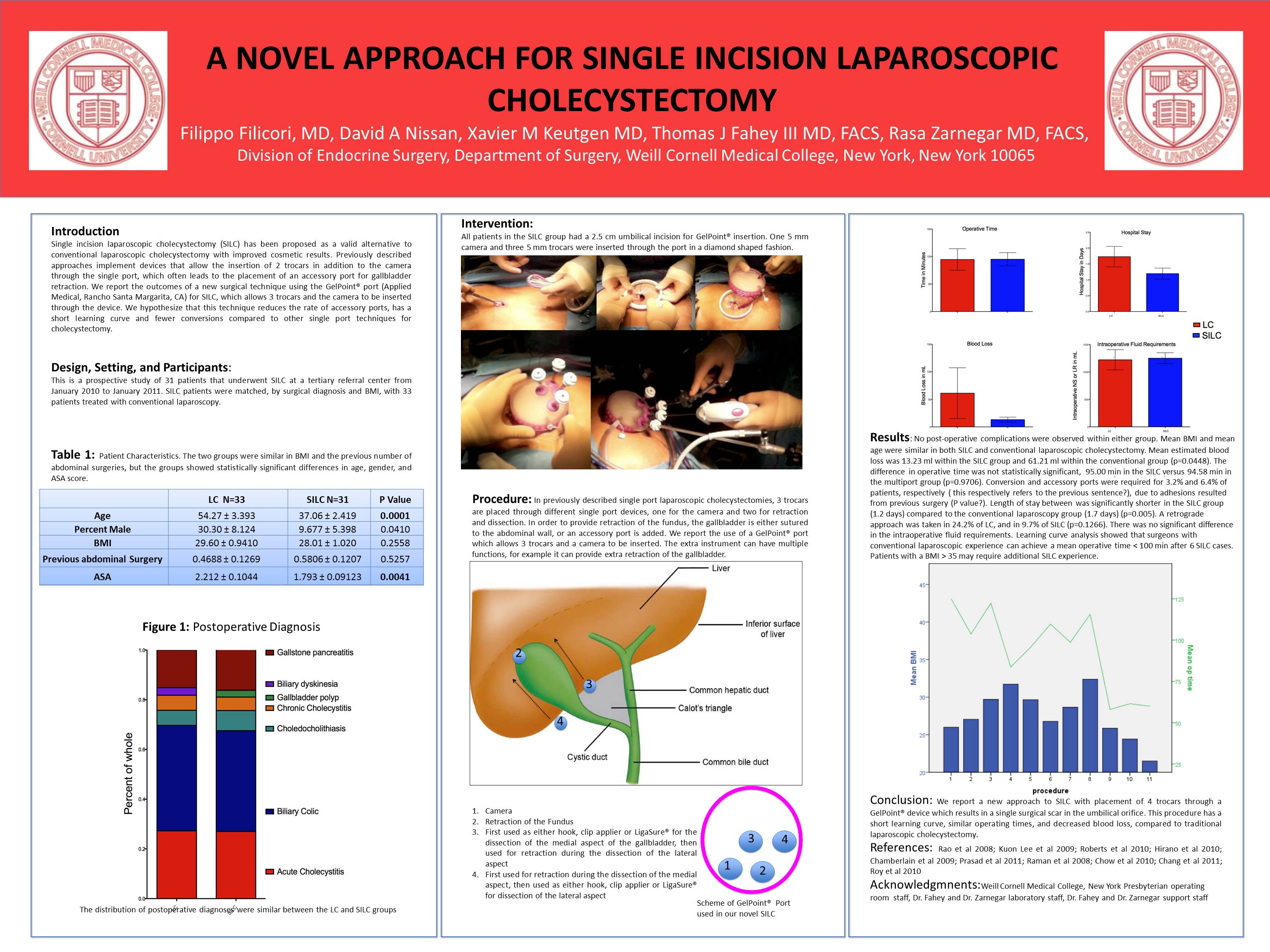
INTRODUCTION: Single incision laparoscopic cholecystectomy (SILC) has been proposed as a valid alternative to conventional laparoscopic cholecystectomy with improved cosmetic results. Previously described approaches implement devices that permit the insertion of 2 trocars in addition to the camera through the single port. Most prior reports require retraction of the gallbladder using an accessory port. We report the outcomes of a new surgical technique using the GelPoint® port (Applied Medical, Rancho Santa Margarita, CA) for SILC, which allows 3 trocars and the camera to be inserted through this device. We hypothesize that this technique reduces the rate of accessory ports, has a short learning curve and fewer conversions than previously reported.
METHODS: This is a prospective study of 16 patients that underwent SILC at a tertiary referral center in 2010. SILC patients were matched, by surgical diagnosis and BMI, with 16 patients treated with conventional laparoscopy. All patients had a 2.5 cm umbilical incision for GelPoint® insertion. One 5 mm camera and three 5 mm trocars were inserted through the port in a diamond shaped fashion.
RESULTS: No post-operative complications were observed within either group. Mean BMI and mean age were similar in both SILC and conventional laparoscopic cholecystectomy. Mean estimated blood loss was 19 ml within the SILC group and 41 ml within the conventional group (p=0.11). Operative time was 108 min in the SILC versus 100 min in the multiport group (p=0.63). Conversion and accessory ports were required for 6.2% and 12.5%, respectively, due to adhesions resulted from previous surgery. There was no difference in the length of stay between the SILC group (1.2 days) compared to the conventional group (1.1 days) (p=0.70). Prior abdominal surgery was present in 62% of the SILC group versus 19% in the conventional group (p=0.01).
Learning curve analysis showed that surgeons with conventional laparoscopic experience could achieve a mean operative time < 100 min after 6 SILC cases. Patients with a BMI > 35 may require additional SILC experience.
CONCLUSIONS: We report a new approach to SILC with placement of 4 trocars through a GelPoint® device. This procedure allows for a short learning curve and has similar outcome to conventional laparoscopy. Patients who had prior abdominal surgery are at increased risk for conversion or placement of accessory ports.
Session: Poster
Program Number: P469
View Poster
{kind=link}